Ah, summertime. Sunny skies, warm weather...some would argue that it’s the best time of the year. However, the arrival of the summer season also brings along with some pesky guests--mosquitos. We are all familiar with these arthropods that bite us and leave us with red, itchy bumps on our skin. While mosquito bites are usually annoying and harmless, mosquitoes can also carry certain diseases that can be transmitted to other hosts through these bites. Some of these diseases, called arboviruses, can be passed to humans; one of these diseases is West Nile Virus.
Back in 1937, a woman from Uganda became the first documented case of West Nile Virus infection. Prior to 1999, West Nile Virus (WNV) was recognized in Africa, the Middle East, Asia, and some European countries. WNV appeared in North America in 1999, when there was an outbreak of the disease in New York City; it has since spread rapidly throughout the United States, as well as parts of Canada and Mexico (Primer, 2002). The U.S. Centers for Disease Control (CDC) has reported more than 30,000 human cases of West Nile Virus since 1999; outbreaks happen every summer and have occurred in at least 48 states (Primer, 2002). In the United States alone, there was a reported 5,674 cases of West Nile Virus in 2012 and 2,469 reported cases in 2013. These statistics do not include the mild cases of West Nile Viruses that have gone unreported; consequently, West Nile Virus is considered to be the most widespread disease in the flavivirus genus it belongs to. The flavivirus name comes from one of the major diseases classified within this genus: Yellow Fever Virus. In Latin, “flavus” means yellow.

States reporting epizootic activity and human infection of West Nile Virus from 1999-2001 (Petersen & Marfin, 2002)
So what exactly is West Nile Virus and how is it characterized? West Nile Virus is a plus-sense, single stranded RNA virus that belongs to the Japanese Encephalitis Antigenic Complex of the Flaviviridae family. West Nile Virus has been detected in humans, more than 100 species of birds, as well as other mammals including horses, dogs, and cats. This blog will primarily focus on West Nile Virus and its relationship to humans.
The typical incubation period, or period between exposure to the infection and appearance of symptoms, is typically between 1-6 days although it can be as long as up to 14 days. However, the majority of people infected with West Nile Virus (approximately 80%) do not show any clinical symptoms (Madden, 2003). About 20-30% of infected people develop West Nile Fever and experience mild symptoms, and less than 1% of infected people develop West Nile neuroinvasive disease in the form of West Nile Encephalitis, Meningitis, Poliomyelitis, or Acute Flaccid Paralysis (Madden, 2003). Around 10% of these cases of West Nile neuroinvasive disease end up being fatal; both the morbidity and mortality rate is higher for individuals older than 50 years of age.
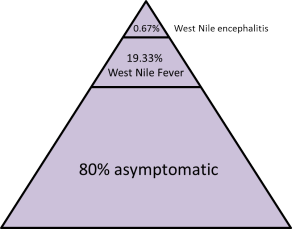
Shives, 2012
For the fortunate middle 20-30% of infected people who develop West Nile Fever, the symptoms are usually so mild that less than 1% of these people actually go to a doctor and are diagnosed. West Nile Fever usually presents as an acute disease, and infected people experience abrupt onset of fever, headache, fatigue, and muscle pain (Madden, 2003). The first symptoms are vague and can also involve a skin rash on the chest, stomach, and back. Other symptoms of West Nile Fever include nausea, vomiting, diarrhea, and other body aches or joint pains. A person that develops West Nile Fever is expected to make a full recovery, although they might experience some fatigue or weakness for weeks or even months (Madden, 2003). It is safe to say that if you were going to be infected with West Nile Virus and develop clinical symptoms, you would want to develop West Nile Fever as opposed to a neuroinvasive form of the disease.
1 out of 150 people infected with West Nile Virus will experience the severe symptoms of West Nile neuroinvasive disease. Neurological symptoms are exacerbated for individuals that have certain pre-existing medical conditions, including cancer, diabetes, hypertension, and kidney disease. The mortality rate for West Nile neuroinvasive disease is about 10%, and those who do survive are in for a difficult recovery; recovery take several weeks to several months, and some people may experience permanent neurologic effects (Lim et al., 2011). When a person is infected with West Nile Virus, the virus multiplies within the person’s bloodstream. Research suggests that the virus first infects the body’s epidermal and dendritic cells, before migrating to regional lymph nodes for replication (Lim et al., 2011). The virus then spreads throughout the body to other organs, including the kidney and spleen, and continues to replicate. Normally, a blood-brain barrier exists to protect the brain and spinal cord from infection; when the blood-brain barrier (BBB) does its job, the infected person will likely develop no symptoms or West Nile Fever (Lim et al., 2011). In rarer cases, in which the virus is able to cross the BBB, West Nile neuroinvasive disease occurs. This small percentage of people that develop a West Nile neuroinvasive disease experience severe symptoms related to West Nile Meningitis (WNM) or West Nile Encephalitis (WNE).
West Nile Meningitis involves inflammation of the membranes surrounding the brain and spinal cord. Symptoms of WNM involve abrupt onset of fever and severe headaches, as well as gastrointestinal symptoms like nausea, vomiting, and diarrhea (Lim et al., 2011). Dehydration and severity of symptoms sometimes requires hospitalization for pain management. Other serious symptoms include nuchal rigidity, or the inability to flex the neck forward, Kernig’s and Brudzinski’s signs, and sensitivity to light and sounds (Lim et al., 2011). Kernig’s signs involve bending of the thigh at awkward angles, painful extensions of the knee, and body spasms. Brudzinski’s signs include involuntary movements of the leg such as flexion and lifting. This type of West Nile neuroinvasive disease usually has a favorable outcome and infected people recover, although persistent headaches, fatigues, and body aches can remain. West Nile Poliomyelitis (WNP) and Acute Flaccid Paralysis (AFP) are also neuroinvasive forms of West Nile Virus characterized by limb and muscle weakness or paralysis. Some individuals with WNP make full recoveries, while others experience persistent limb weakness or pain (Lim et al., 2011). In severe cases of WNP, infected people can suffer from respiratory failure due to respiratory muscle disruption by the virus. Recovery from the severe forms of WNP are more difficult and are associated with high rates of mortality; those that do survive usually need intensive hospital care for many months.
West Nile Encephalitis, or inflammation of the brain, is the more serious of West Nile neuroinvasive diseases and is most commonly seen in individuals over the age of 55 and immunocompromised individuals (Lim et al., 2011). Symptoms of WNE can range from being mild and involving self-limited states of confusion, to causing severe brain damage, malfunctioning, coma, and death (Lim et al., 2011). Common symptoms of WNE include tremors in the upper extremities, involuntary jerks of the upper extremities and facial muscles, Parkinson’s disease-like decreases in facial expressions, and difficulty with balance and overall body movement. People suffering from WNE can also experience depression, anxiety, and apathy (Lim et al., 2011). The prognosis for WNE varies and depends on the individual, the mortality rate is higher for immunocompromised and older people, and some people also are observed to make full recoveries.

Average annual incidence of West Nile virus neuroinvasive disease by age group and clinical syndrome in the U.S. 2008 by the Centers for Disease Control, 2010
Diagnosing West Nile Virus relies on both clinical symptoms, as well as laboratory tests that can isolate the virus or detect WNV-specific antibodies in a person’s blood or cerebrospinal fluid (CSF) (Sejvar, 2014). Most commonly, antibody testing is used to detect immunoglobulin WNV antibodies, which are detectable from 3-90 days after onset of illness, in blood or CSF. Detection of antibodies can be done through enzyme-linked immunosorbent assays, known as ELISA assays, that measure the concentration of antibodies (Sejvar, 2014). Plaque reduction neutralization tests (PRNTs) are also used to diagnose WNV infections, such as West Nile Meningitis, to detect changes in the amount of WNV-specific antibodies and white blood cells in a person’s blood or CSF. A fourfold or greater change in these antibodies suggests the presence of infection. Methods of isolating West Nile Virus RNA in tissues, blood, or CSF are also used to confirm infection. These methods include viral cultures or reverse transcriptase-polymerase chain reactions (RT-PCR), and immunohistochemistry analyses (Sejvar, 2014).
One of the positive consequences of contracting West Nile Virus is that these antibodies and T-lymphocyte white blood cells produced to fight the infection will stay in your body for a long time. These antibodies and white blood cells will protect you from future infections of the virus and it is currently assumed that you have lifelong immunity after contracting WNV once; however, this immunity does decrease as time since the infection passes. As you can see, West Nile Virus is no joke--it can have mild consequences or cause life-threatening illnesses. If you live in an area where West Nile Virus has been documented in mosquitoes, I hope that you remember the importance of staying protected from mosquitoes this summer. Not only will this protect you from those pesky, itchy mosquito bites, but it could also save your life. The next blog posts will talk more about how to protect yourself from West Nile Virus and prevent its spread, as well as how the disease is transmitted and leads to seasonal outbreaks.
References
Hoenen, A., Gillespie, L., Morgan, G., van der Heide, P., Khromykh, Al, & Mackenzie, J. (2014). The West Nile virus assembly process evades the conserved antiviral mechanism of the interferon-induced MxA protein. Virology, 448, 104-116. doi: 10.1016/j.virol.2013.10.005
Lim, S., Koraka, P., Osterhaus, A., & Martina, B. (2011). West Nile Virus: Immunity and Pathogenesis. Viruses, 3(6), 811-828
Petersen, L., & Marfin, A. (2002). West Nile Virus: A Primer for the Clinician. Annals of Internal Medicine, 137(3), 173-179. doi: 10.736/0003-4819137-3-200208060-00009
Sejvar, J. (2014). Clinical Manifestations and Outcomes of West Nile Virus Infection. Viruses, 6(2), 606-623
No comments:
Post a Comment