One Mosquito Bite Can Change a Life Forever [Motion Picture]. (2014). United States: American Mosquito Control Association.
The American Mosquito Control Association (AMCA) created the short documentary video above as part of their “I’m One” Outreach Program. This program is aimed at encouraging individuals to proactively find opportunities to prevent the spread of mosquito-borne diseases in their community and draw attention to the threat of West Nile Virus in particular. Ultimately, the AMCA’s mission is to spread the message about the necessity for mosquito control, protection, and prevention.
This video is very powerful to watch and does a great job of helping the public better understand West Nile Virus, its threats, and what individuals can do to prevent risk of infection. The video starts off by giving statistics on the number of mosquito born illnesses reported in the year of 2012 in the United States, which is over 5,600. 286 of these cases were fatal according to the video; these statistics really send a message that mosquito bites can be more than just a pesky itch and cause serious, life threatening diseases. One of the most impactful aspects of the video are the personal stories shared by individuals who have suffered from West Nile Virus and experienced the devastating side effects of the more severe forms of the disease. One of the individuals infected was an older man that was a surgeon, and another was a middle-aged man that had lived a very healthy and active lifestyle prior to becoming infected. Both of these individuals shared their experiences with the abrupt onset of neuroinvasive diseases that lead to muscle weakness, paralysis, and excruciating pain. The two men shared how the recovery process was incredibly difficult and slow; one had to take off work for more than 7 months and the was hospitalized for an entire year. These stories highlight the dangerous complications from WNV and also emphasize the long-term consequences of the disease. The individuals in the video, who have since recovered from WNV, talk about the lifelong persistent impairments they suffer from to this day. They both had to relearn how to walk, and continue to experience fatigue, muscle weakness, and difficulties with physical control of their movements. One of the men can longer longer run and requires support for mobility through walking. Another story shared in the video is by a woman who lost tragically lost her young child to West Nile Virus. Her child began to show symptoms and passed away 6 days later. This particular story emphasized the possibility for mosquito-borne illnesses like West Nile Virus to be virulent and deadly. The woman also mentioned the large medical expenses that attributed to medical treatments; her statements were supported by the men who said they had to face incredible medical expenses as a result of their long hospital stays and continual physical therapy and rehabilitation.
Overall this video did a good job of highlighting the nature of this virus; primarily, the video stressed that this virus can happen to anyone and everyone is susceptible and at risk. The stories featured people of very different demographics, including a young girl, an older man, and a middle aged man that all were infected with WNV. I think that this aspect of the video helps to combat people’s notions that this situation will not happen to them. In addition, the video highlights the far-reaching impacts of WNV on not only an individual’s health, but also the economy and their families for the rest of their lives. The video also mentioned the importance of taking prevention measures in the community to control mosquito populations and discourage breeding in the area.
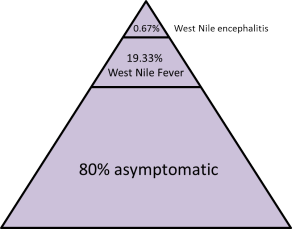
While I believe this video is very effective in raising awareness of the potential serious consequences of mosquito-borne illnesses, I think it would have been beneficial for the video to talk about more ways people can contribute to mosquito surveillance in their community. Surveillance is an important part of keeping track on the spread of WNV and reporting dead birds or other animals to surveillance agencies can be crucial indicators of impending outbreaks of the virus in communities. The video also does not mention individuals who are at higher risk for the more serious aspects of the disease and who should be especially care, including young children, immunocompromised individuals, and especially elderly persons over the age of 70. I also believe that it would be helpful to not only touch upon the severe neuroinvasive cases of the disease, but to inform the public about the fact that about 80% of infected people are asymptomatic and the majority of symptomatic individuals display signs of West Nile Fever. I believe it is important for people to know that they may have WNV or experience WNF without even knowing it because of febrile-like symptoms of the illness. This is important because this would make individuals more aware of the role they could play in accurate surveillance of incidence reports of the disease. If the video provided information on the more vague symptoms of WNV and also emphasized the issue of underreporting and inaccurate surveillance of WNV cases, people would be more likely to address this issue by obtaining diagnosis for their symptoms and reporting their cases to the CDC. This type of awareness would also stress to the public the gravity of the risk and the widespread nature of mosquito-borne illnesses due to their ease of transmissibility.
Despite these small additions I would make to the documentary, I really encourage you to share this informative video with your friends and family to help spread awareness about West Nile Virus! The more educated people are about the risks and how WNV could directly impact them, the more likely they will be to learn more about ways they can help to prevent the spread of the virus and protect themselves, as well as their community.
For more information about preventing mosquito-borne diseases like West Nile Virus, you can visit the American Mosquito Control Association’s website (where the video is originally from):